
MBBS · FCPS · Internationally Trained · ESCP · FASCRS • 13,000+ Patients Treated • Same-Day Discharge • Hill Park General Hospital
Fistula Treatment in Karachi | Laser Surgery | Dr. Abdullah Iqbal
Last updated: June 27, 2026 · Reviewed by Dr. Abdullah Iqbal, MBBS, FCPS
Book a Direct Consultation with Dr. Abdullah Iqbal
Speak directly with Dr. Abdullah Iqbal. No third-party booking platforms.
Your information is confidential and used only to schedule your consultation. See our Privacy Policy.
Prefer to talk now? 0333-2877351 • WhatsApp
How is fistula treated with laser surgery in Karachi?
Fistula (bhagandar) is treated with FiLaC laser surgery — a sphincter-safe procedure where a laser fiber closes the fistula tract from inside without any external cuts or open wounds. Dr. Abdullah Iqbal, Pakistan’s first laser proctologist, performs this procedure at Karachi Piles Clinic, Hill Park General Hospital. Same-day discharge, 5–7 day recovery, and no risk of incontinence. Over 5,000 laser procedures performed.
Fistula Treatment in Karachi — Laser Surgery by Dr. Abdullah Iqbal
| Condition | Anal Fistula (Bhagandar — بھگندر) |
| Specialist | Dr. Abdullah Iqbal — MBBS, FCPS, Laser Proctologist, Karachi |
| Techniques Available | FiLaC, LIFT, VAAFT, Fistulotomy, Fistulectomy, PILTEC, Fistula Plug |
| Laser Surgery Cost | PKR 150,000 – 250,000 (depending on complexity) |
| Open Surgery Cost | PKR 70,000 – 80,000 |
| Recovery (Laser) | 3–5 days to routine | Full healing 4–8 weeks |
| Recovery (Open) | 4–6 weeks with wound dressings |
| Location | Karachi Piles Clinic, Hill Park General Hospital & MediCenter, Karachi |
| Last Reviewed | March 2026 by Dr. Abdullah Iqbal |
Anal fistula (bhagandar) is a chronic anorectal condition that requires surgical treatment — it does not resolve on its own. Dr. Abdullah Iqbal is a laser proctologist in Karachi with 13+ years of experience, holding MBBS and FCPS qualifications, and has performed more than 5,000 laser proctology procedures including complex fistula surgeries using FiLaC, LIFT, VAAFT, and PILTEC techniques.
Every week I meet patients who have been silently suffering from a fistula for months or even years — delaying treatment out of embarrassment or hoping it will heal on its own. I want to be clear: with the right diagnosis and the right technique, anal fistula is very treatable, and laser surgery today means most patients go home the same day with minimal pain and a fast recovery. If you are looking for fistula treatment in Karachi, you are in the right place.
I trained in general surgery, then specialised in colorectal surgery and laser proctology. I have treated thousands of fistula cases — from simple intersphincteric tracts to high complex horseshoe fistulas that had recurred after previous surgery elsewhere. My team and I at Karachi Piles Clinic, Hill Park General Hospital are here to help you get a permanent solution.
What is Anal Fistula?
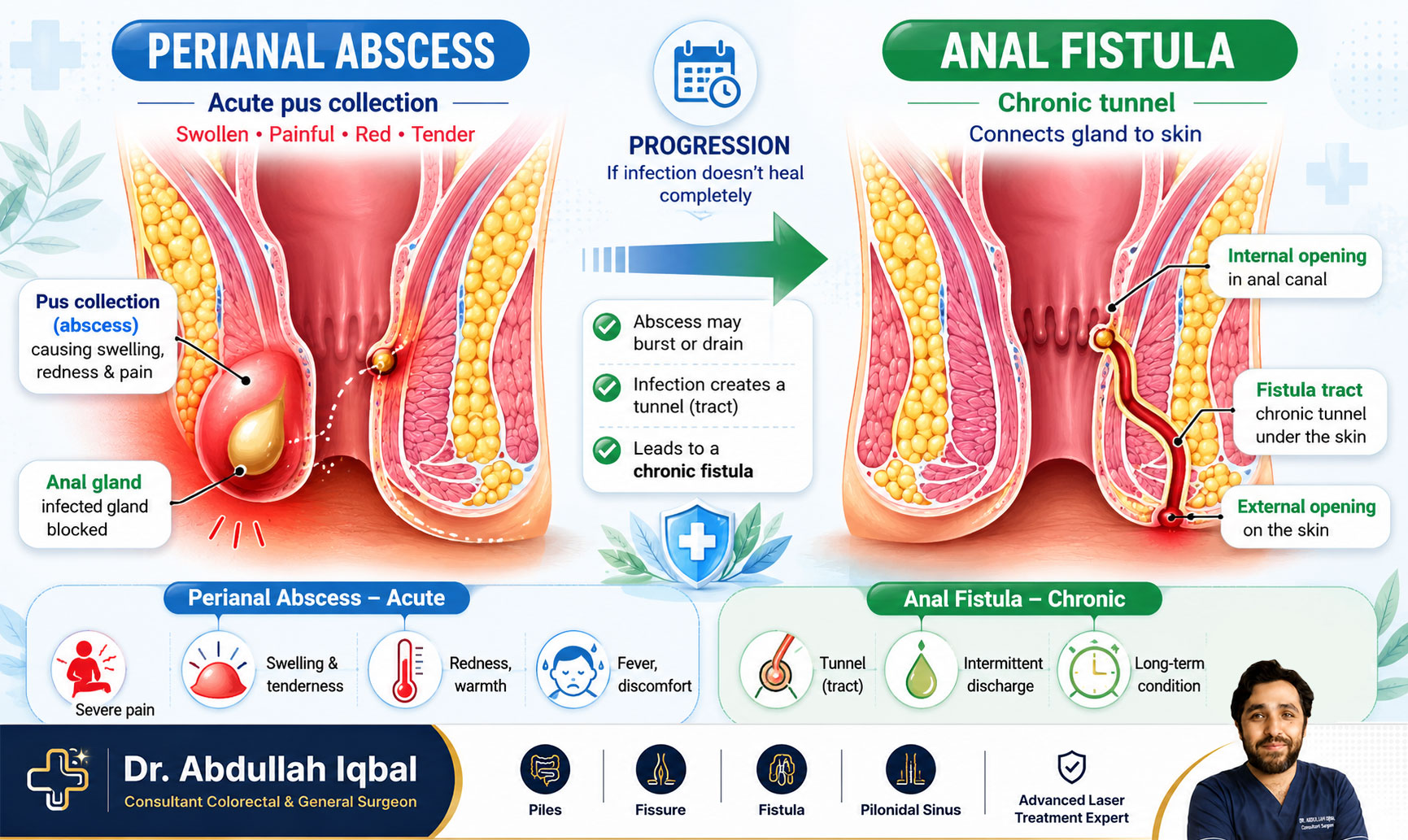
A fistula is an abnormal tunnel that forms under the skin, connecting the inside of the anal canal or rectum to an opening on the skin near the anus. Most people develop it after an anal abscess (a pocket of infection and pus). Approximately 50% of perianal abscesses go on to form a fistula tract if not fully treated.
Sometimes a fistula develops gradually without a clear abscess episode. The hallmark sign is a small opening near the anus that persistently drains pus, blood, or foul-smelling fluid. A fistula tract has a lined wall that the body cannot close on its own — the tract must be surgically cleared or sealed for permanent healing.
Types of Anal Fistula
Fistulas are classified based on their relationship to the anal sphincter muscles — the muscles that control bowel continence. This classification is critical because it directly determines which surgical technique is safest for your specific case. I map every fistula using MRI before planning treatment.
Types of Fistula in Ano (Parks Classification)
- Intersphincteric — Runs between the inner and outer sphincter muscle layers. Most common type. Usually a simple fistula suitable for single-stage laser treatment.
- Transsphincteric — Passes through part of the outer sphincter muscle. Complexity depends on how much muscle is involved.
- Suprasphincteric — Curves high above the sphincter complex before exiting. High fistula requiring careful two-stage approach.
- Extrasphincteric — Very rare. Usually results from pelvic injury, inflammatory bowel disease, or previous surgery.
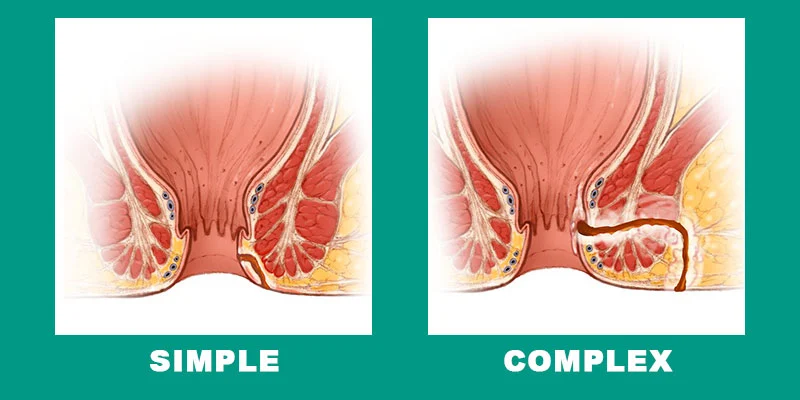
Simple vs Complex Fistula — What Is the Difference?
Another important classification divides fistulas into simple and complex based on tract size, number of openings, sphincter involvement, and treatment history. This distinction directly determines whether a one-stage or two-stage surgical approach is needed.
Simple Fistula: A low-lying tract that crosses little or no sphincter muscle — typically less than one-third of the external sphincter. All intersphincteric fistulas and low transsphincteric fistulas involving less than 30% of the external sphincter are classified as simple. These are suitable for single-stage laser treatment with excellent outcomes.
Complex Fistula: A high, multi-branched, or recurrent fistula that involves significant sphincter muscle and carries a risk of incontinence if treated aggressively in one sitting. A fistula is classified as complex if it meets any of the following criteria:
- Involves more than 30% of the external sphincter
- Has recurred after previous surgery
- Has multiple branches or a horseshoe configuration
- Is associated with Crohn’s disease, tuberculosis, prior pelvic radiation, or pre-existing incontinence
- In women: anterior (front-side) fistulas are also considered complex because the sphincter is thinner anteriorly
I always determine simple versus complex classification at your first visit so I can explain clearly which treatment pathway is safest for you.

Symptoms of Anal Fistula
If you are reading this, you may already be experiencing one or more of the following. These are the most common symptoms that bring patients to my clinic for fistula assessment:
- Persistent pain and swelling near the anus, often worse when sitting
- Pus, blood, or yellow discharge from a small opening near the anus
- Skin irritation and itching around the anal area
- Pain during or after passing stool
- Recurrent feeling of fever or tiredness when infection flares
- A swelling near the anus that bursts and gives temporary relief, then re-forms
If these symptoms recur, do not delay. Early treatment of a fistula is almost always simpler, less expensive, and more successful than treating a fistula that has been left to enlarge or develop branches. Book an appointment for an assessment.
What Causes Anal Fistula?
Understanding the cause of your fistula is important — it helps treat any underlying condition and reduces the risk of recurrence after surgery.
Blocked Anal Glands (Most Common): Small glands inside the anal canal can become blocked and infected, forming an abscess that eventually burrows through tissue to create a fistula tract.
Unresolved Perianal Abscess: If a perianal abscess is not properly drained — or if it was drained but the underlying gland was not addressed — a fistula tract typically forms as the body creates a persistent drainage channel. Around half of all perianal abscesses lead to fistula formation.
Other causes include:
- Inflammatory bowel disease such as Crohn’s disease — associated with complex, recurrent fistulas
- Irritable bowel syndrome
- Tuberculosis — more common in Pakistan and should be excluded in all fistula patients
- Radiation for pelvic cancers
- Injuries, obstetric tears, or previous anorectal surgery
- Sexually transmitted infections
- Rarely, rectal or anal cancer
During your consultation, I take a thorough history specifically looking for bowel symptoms, weight loss, night sweats, or prior illness that may point to an underlying cause that needs to be treated alongside the fistula.
How I Diagnose Fistula at My Clinic
Accurate diagnosis and complete mapping of the fistula tract is the most critical step — it is what determines which technique will give you the best outcome with the least risk.
I examine you gently in a private setting using a gloved finger to assess the external opening, check for discharge, and feel for the subcutaneous cord. I then use a small anoscope to inspect the internal opening inside the anal canal.
For complex or branching tracts, I order an MRI fistulogram — the gold standard imaging investigation that provides a precise three-dimensional map of the tract’s length, depth, and relationship to the sphincter muscles. For patients where I suspect underlying inflammatory bowel disease, I may also order a colonoscopy or blood tests including TB workup.
Thorough pre-operative mapping is what separates a successful fistula surgery from one that recurs. I never operate on a fistula without knowing exactly what I am dealing with.
Fistula Treatment Options in Karachi
Fistula does not heal without surgery. The fundamental goal of all fistula surgery is to eliminate the infected tract while protecting the anal sphincter muscles and preserving bowel continence. The method I recommend depends on the type and complexity of your fistula, your overall health, and your history of any previous fistula treatment.
At my clinic I use both standard open techniques and laser-assisted fistula surgery. For the large majority of patients, a laser-based approach offers less post-operative pain, faster return to normal activities, and no need for wound dressings.
Key surgical considerations I discuss with every patient:
- Pain — Modern laser techniques result in significantly less post-operative pain than traditional open surgery.
- Bleeding — Laser seals blood vessels during treatment; heavy post-operative bleeding is rare.
- Wound care — Laser procedures generally require no dressings; sitz baths twice daily are sufficient.
- Recurrence — Complete MRI mapping and meticulous surgical technique keep recurrence rates low.
- Continence — Preserving sphincter function is my primary concern in all fistula cases, especially complex ones.
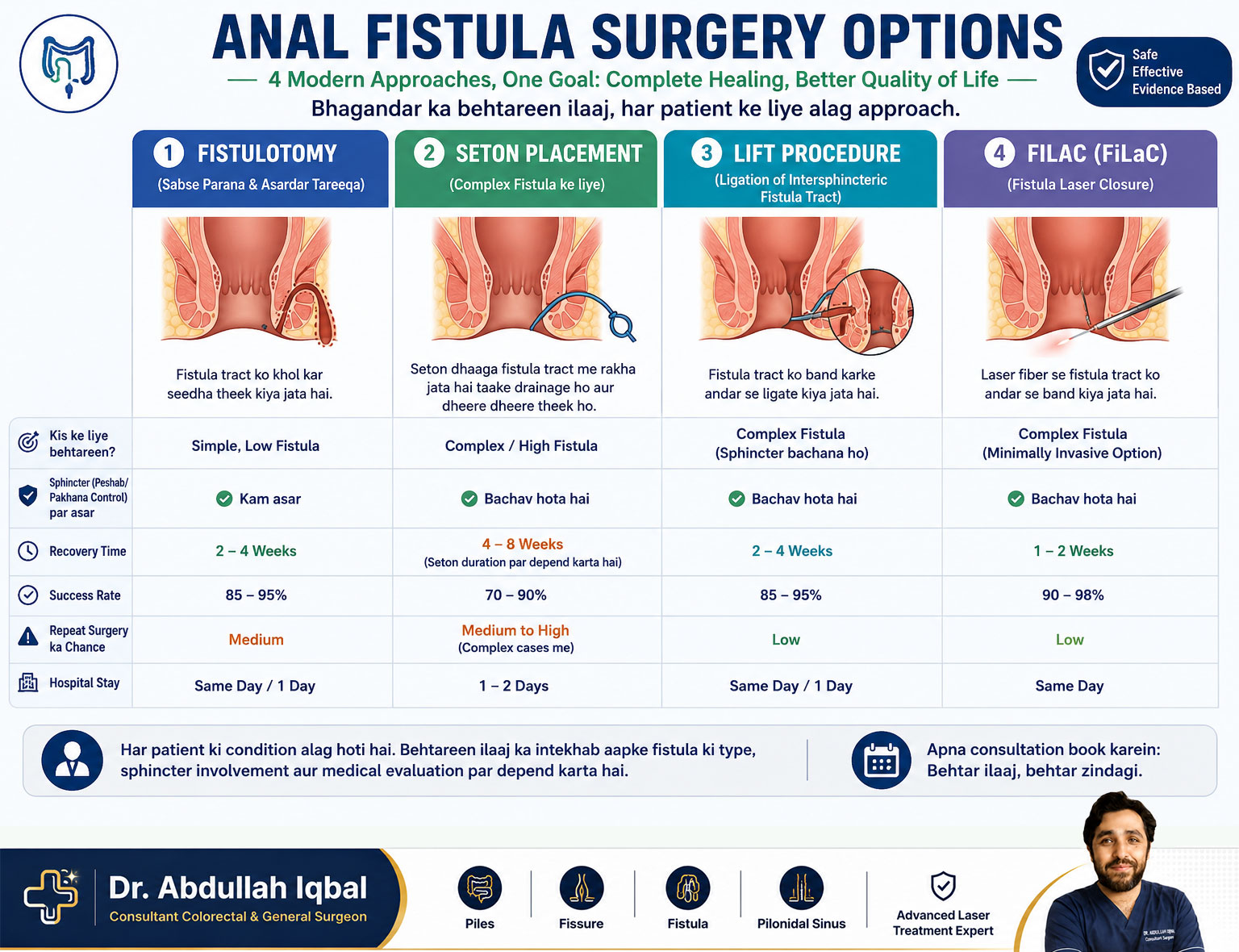
1. Fistulotomy
I open the entire fistula tract along its length, allowing it to heal flat from the base as a scar. Fistulotomy is the simplest technique with the highest success rate for low, simple fistulas involving minimal sphincter muscle. It is not appropriate when significant muscle is at risk.
2. Fistulectomy with Laser
I excise the entire fistula tract and use laser energy to seal the edges, reducing bleeding and accelerating healing. This is suitable for simple fistulas where complete removal of the infected tract is desired.
3. LIFT — Ligation of the Intersphincteric Fistula Tract
LIFT is an excellent sphincter-sparing technique for transsphincteric fistulas. I access the intersphincteric plane, ligate (tie off) the internal opening, and curettage the outer portion — without cutting any sphincter muscle. I also perform Laser-assisted LIFT (LIFT + FiLaC) for superior closure rates.
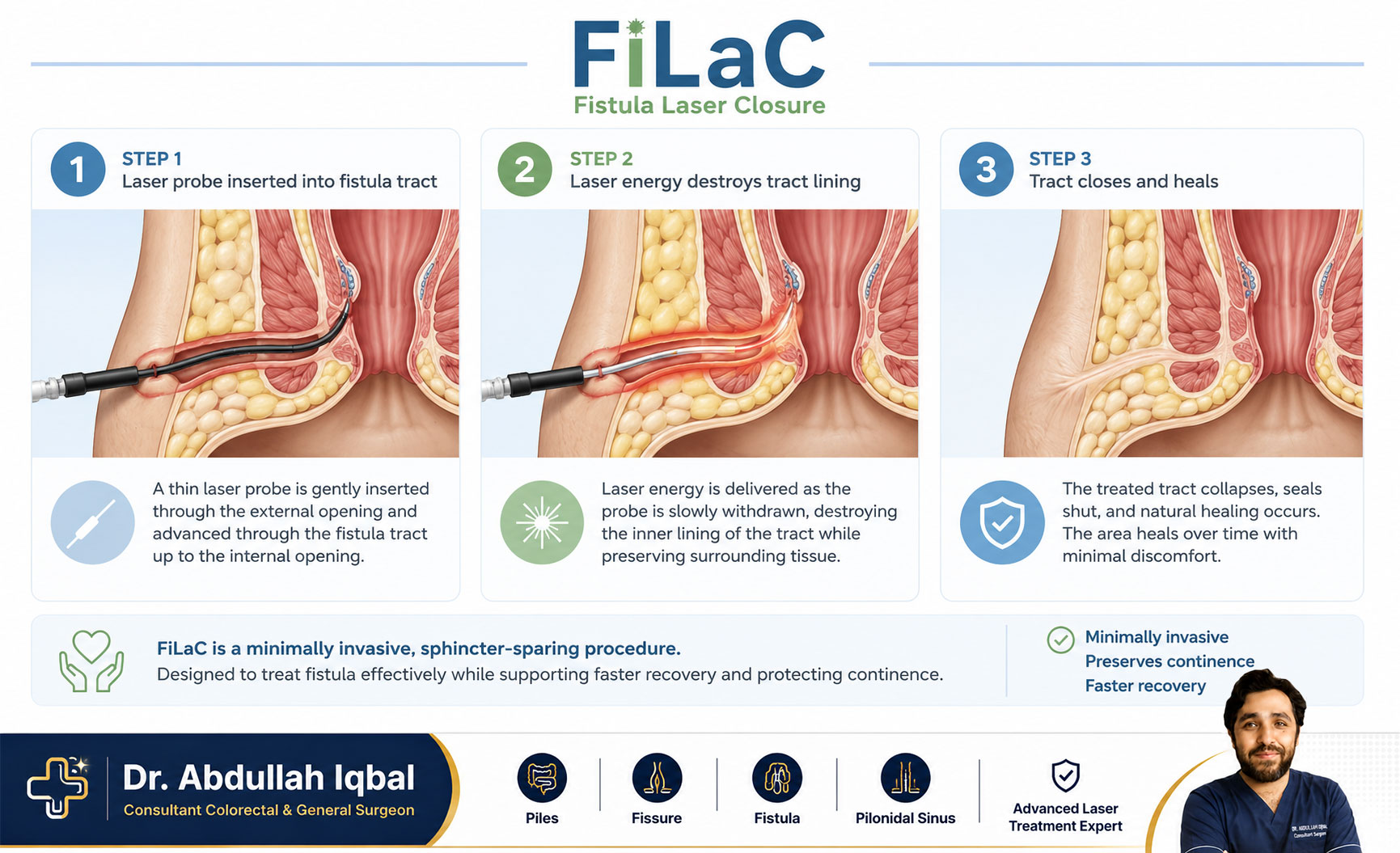
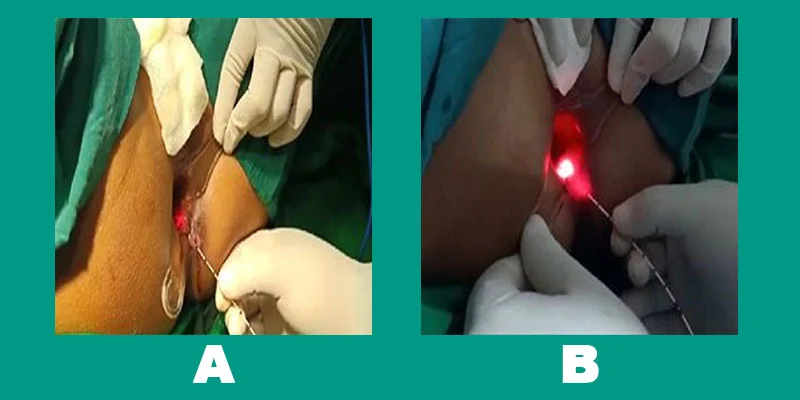
4. FiLaC — Fistula Laser Closure
A precision radial-emitting laser fiber is passed through the external opening and advanced along the entire fistula tract. The laser energy destroys the tract lining from within and seals it shut. There is no external cut, no wound to dress, and patients typically return home the same day. FiLaC success rates exceed 90% for simple fistulas in experienced hands.
5. VAAFT — Video-Assisted Anal Fistula Treatment
I insert a thin fistuloscope to directly visualise the inside of the tract, cauterise it under vision, and close the internal opening with sutures. The outer skin remains intact. VAAFT has a recurrence rate of approximately 30% but remains a valuable option for selected complex cases where preserving tissue is the priority.
6. Fistula Plug
A bio-absorbable plug made from porcine or synthetic material is inserted into the fistula tract. The body gradually grows tissue around it. The procedure is nearly painless with minimal recovery, but plug displacement or infection remains a limitation in some cases.
7. PILTEC
A technique I use for very complex, multi-branched, or recurrent fistulas. PILTEC is an advanced evolution of LIFT combined with laser steps that I studied under international experts. I have achieved consistent results with this technique even in cases that had failed previous surgeries elsewhere.
One-Stage vs Two-Stage Procedure
Whether your fistula is treated in one sitting or two depends entirely on its complexity.
One-Stage Procedure: Ideal for simple, low fistulas with a single straight tract. The entire fistula is treated in a single operation — typically with FiLaC (Fistula Laser Closure) or laser-assisted fistulectomy. Healing is faster and post-operative discomfort is minimal.
Two-Stage Procedure (For Complex Fistulas): If your fistula is high, has multiple branches, or involves significant sphincter muscle, a two-stage approach protects continence and improves long-term results:
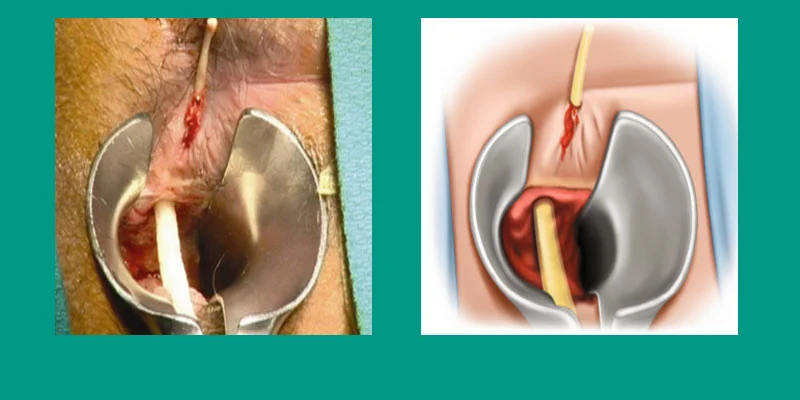
- Stage 1 — Seton Placement: A special medical-grade thread (seton) is placed through the fistula tract. It either drains the infection and keeps the area dry (draining seton), or gradually divides deep tissue without damaging muscle (cutting seton). This stage settles inflammation and prepares the tract for definitive closure.
- Stage 2 — FiLaC Laser Closure: Once the area has settled and infection resolved, I perform laser closure using a precision radial fiber. Laser energy seals the tract lining, reduces infection risk, and preserves continence. Using laser in both stages gives superior outcomes and faster return to daily life compared to conventional two-stage surgery.
Why Choose Laser for Fistula Treatment?
- Precision: Laser energy is controlled to millimeter accuracy, treating the fistula tract while protecting surrounding healthy tissue and sphincter muscle.
- Less Pain: Laser fistula procedures result in significantly less post-operative pain than traditional open surgery — most patients manage with simple oral painkillers only.
- Faster Recovery: Return to normal daily activities within 3 to 5 days, compared to 4 to 6 weeks with open surgery.
- No Dressings: Laser seals the wound internally — there are no open wounds requiring packing or dressing changes.
- Lower Infection Risk: The laser’s thermal energy has antimicrobial properties, reducing post-operative infection rates.
- Sphincter Preservation: Laser-based techniques protect the anal sphincter muscles, maintaining continence — the most important functional outcome.
- Day Surgery: Most laser fistula procedures are performed as day-care operations, meaning you go home the same day.
Fistula Surgery Cost in Karachi — Complete Breakdown
Laser fistula surgery with Dr. Abdullah Iqbal ranges from PKR 150,000 to PKR 250,000. The final amount depends on the following factors:
Factors That Affect Fistula Surgery Cost
- Type and Complexity: Simple single-tract fistulas cost less than complex high or horseshoe fistulas requiring multi-stage treatment.
- Single-Stage vs Two-Stage: A two-stage procedure involves two separate operating sessions, which increases total cost.
- Laser Fiber Quality: The single-use imported laser fiber accounts for approximately 60% of the surgical cost. We use only high-quality precision fibers — this directly determines your outcome.
- Hospital and Theatre: Fees vary between Hill Park General Hospital and MediCenter based on room type and theatre setup.
- Anaesthesia: General or spinal anaesthesia and the required monitoring also contribute to the total.
Open conventional fistula surgery in Karachi costs approximately PKR 70,000 to 80,000. However, open surgery involves longer hospital stay, painful wound dressings for 4 to 6 weeks, and a significantly longer recovery period.
Summary of Estimated Costs
The cost of fistula surgery in Karachi depends on the type and complexity of the case. Laser surgery is more advanced and costs higher, while open surgery is less expensive but requires longer recovery.
Fistula surgery is covered under most insurance plans.
Both FiLaC and LIFT procedures are classified as inpatient surgical procedures and qualify for coverage under EFU, Jubilee, Adamjee, IGI, State Life and other major Pakistani panels. See the full list of accepted insurance providers and how the pre-authorization works — we handle the verification with your insurer directly.
After Surgery — Recovery and Preventing Recurrence
Why Fistulas Come Back
Fistula recurrence most commonly occurs when a branch of the tract was missed during surgery, when underlying infection was not fully resolved, when an underlying cause such as Crohn’s disease or tuberculosis was not identified and treated, or when post-operative care was inadequate. This is why I always perform MRI mapping before surgery and follow every patient personally until complete healing is confirmed.
Post-Operative Care — How to Heal Well
- Sitz baths (warm water with antiseptic) for 15 to 20 minutes, 2 to 3 times daily and after every bowel movement
- Clean with water after each bowel movement — avoid rough toilet tissue
- Apply prescribed ointment gently as instructed
- High-fibre soft diet: papaya, apple, boiled vegetables, daal, oats
- Drink 10 to 12 glasses of water daily — more during Karachi’s summer months
- Use a prescribed stool softener at night for the first few weeks
- Avoid heavy lifting and strenuous exercise until the wound is fully closed
- Contact me immediately if you experience severe pain, high fever above 38.5°C, or heavy bleeding
Most patients return to routine within 3 to 5 days of laser surgery. Full internal healing takes 4 to 8 weeks. I see every patient personally at their follow-up visits until healing is complete. For a detailed guide on what to expect, read our expert advice on fistula surgery and recovery.
Why Choose Dr. Abdullah Iqbal for Fistula Surgery in Karachi
Choosing the right surgeon for fistula treatment matters enormously — an incomplete or poorly planned operation is the most common reason fistulas recur. Here is what makes my approach different:
- Dedicated anorectal practice: I focus exclusively on piles, hemorrhoids, fissure, and fistula — this is not a general surgery side practice
- Over 1,000 laser fistula procedures performed annually, including complex recurrent cases
- One of the leading practitioners of laser fistula surgery in Pakistan — trained in FiLaC, VAAFT, PILTEC, and Laser-LIFT techniques
- Pre-operative MRI fistulogram performed on all complex cases — I do not operate without a map
- Hospitals located at Hill Park General Hospital (near Shahid-e-Millat Road) and MediCenter — easily accessible from Bahadurabad, Tariq Road, and PECHS
- International-standard laser equipment using imported, high-quality single-use fibers
- Personal follow-up: I see every patient myself at every visit until they are fully healed
- Also specialises in anal fissure laser treatment and hemorrhoid surgery for patients with multiple anorectal conditions
Living With Fistula — Do Not Delay Treatment
An untreated anal fistula is not merely a small inconvenience — it is an active, ongoing infection that can spread, form new branches, develop into a complex horseshoe fistula, or cause a large perianal abscess requiring emergency surgery. Some patients have been draining pus for years, and by the time they reach me the tract has become significantly more complex than it was at the start.
I understand the embarrassment around these conditions. I deal with this every day and my clinic maintains complete patient privacy at all times. Every patient is treated with respect and dignity. Please do not wait until your fistula becomes a surgical emergency. Book a consultation — an early, simple fistula is almost always treatable in a single laser session.
Frequently Asked Questions — Fistula Treatment in Karachi
What is the cost of fistula laser surgery in Karachi?
Laser fistula surgery in Karachi costs between PKR 150,000 and PKR 250,000. Simple single-stage fistulas typically cost PKR 150,000 to 180,000. Complex or two-stage fistulas requiring seton placement followed by FiLaC laser closure range from PKR 200,000 to 250,000 or more. The laser fiber itself accounts for approximately 60% of the surgical cost as it is a single-use imported device. Open conventional fistula surgery costs PKR 70,000 to 80,000 but requires significantly longer recovery with wound dressings for 4 to 6 weeks.
How long does recovery take after fistula surgery?
After laser fistula surgery, most patients return to normal daily activities within 3 to 5 days. Complete internal healing typically takes 4 to 8 weeks depending on fistula complexity. Open conventional surgery requires 4 to 6 weeks before returning to normal activities, with wound dressings needed throughout that period. Laser procedures eliminate the need for dressings and significantly reduce post-operative pain compared to traditional surgery.
Will I need time off work after fistula surgery?
Office workers and desk-job employees typically need 3 to 7 days off after laser fistula surgery. Patients with physically demanding jobs — labourers, those who stand for long hours, or those who drive long distances — may need 2 to 3 weeks. Most laser fistula procedures are performed as day-care operations, meaning patients are discharged the same day without hospital admission.
Can fistulas be prevented?
Not all anal fistulas can be prevented, but risk can be reduced significantly. The most effective prevention is prompt and proper treatment of perianal abscesses before they form a fistula tract. Managing underlying conditions such as Crohn’s disease, tuberculosis, or inflammatory bowel disease also lowers fistula risk. Maintaining a high-fibre diet, good anal hygiene, and adequate hydration supports overall anorectal health.
Are there non-surgical options for anal fistula?
No. Anal fistulas do not heal without surgical intervention. The fistula tract has a lined epithelial wall that the body cannot close spontaneously. Antibiotics may temporarily reduce associated infection or discharge but will not close the tract. Creams, home remedies, and herbal treatments provide no cure. For a detailed look at what does and does not work, read our article on healing a fistula without surgery. Surgical intervention — whether fistulotomy, laser FiLaC, LIFT, or VAAFT — is the only definitive treatment for anal fistula.
What is the success rate of fistula surgery?
Success rates depend on procedure type and fistula complexity. For simple fistulas treated with FiLaC laser closure, success rates exceed 90 to 95%. For complex fistulas managed with a two-stage LIFT plus laser approach, rates remain between 85 and 95% in experienced hands. VAAFT has a recurrence rate of approximately 30% but remains suitable for selected complex cases. In my practice, recurrence rates for laser procedures are consistently below 5%.
What are the chances of fistula coming back after surgery?
With complete pre-operative MRI mapping and meticulous surgical technique, recurrence rates are less than 5% for simple fistulas and less than 10 to 15% for complex multi-branched cases. The most common causes of recurrence are a missed branch of the tract, an untreated underlying condition such as Crohn’s disease or tuberculosis, or inadequate post-operative care. I perform MRI fistulogram on all complex cases before surgery specifically to minimise this risk.
Related Proctology Conditions
Many patients have overlapping symptoms across these conditions. If your symptoms point toward something else, here are the other proctology procedures I perform at Karachi Piles Clinic:
- Laser Fissure Treatment — painless sphincterotomy for chronic anal fissures, includes conservative options (GTN cream, Xyloaid, sitz baths).
- Laser Pilonidal Sinus Treatment — minimally invasive laser sinus closure near the tailbone.
- Laser Piles Treatment — bloodless day-care hemorrhoidectomy by Pakistan’s first laser proctologist.
Not sure which condition you have? Try our Self-Diagnosis Tool or WhatsApp directly: 0333-2877351
Medical Disclaimer: The information on this page is for educational purposes only and does not constitute medical advice. Consult Dr. Abdullah Iqbal directly for diagnosis and treatment.
Trusted Medical References
For more on this topic in your own language, see Dr. Abdullah’s guide to Bhagandar Ki Alamaat (fistula symptoms in Roman Urdu). If you’re trying to understand whether what you have is a fistula or an abscess, our comparison piece on fistula vs abscess walks you through the key differences.
For international clinical perspectives, see:
- Mayo Clinic — Anal Fistula
- NHS UK — Anal Fistula
- Cleveland Clinic — Anal Fistula
- NCBI StatPearls — Anal Fistula (peer-reviewed)
Worried about a possible fistula or abscess?
Dr. Abdullah Iqbal — Pakistan’s first laser proctologist — has performed 1,500+ laser procedures. Share your symptoms confidentially on WhatsApp.